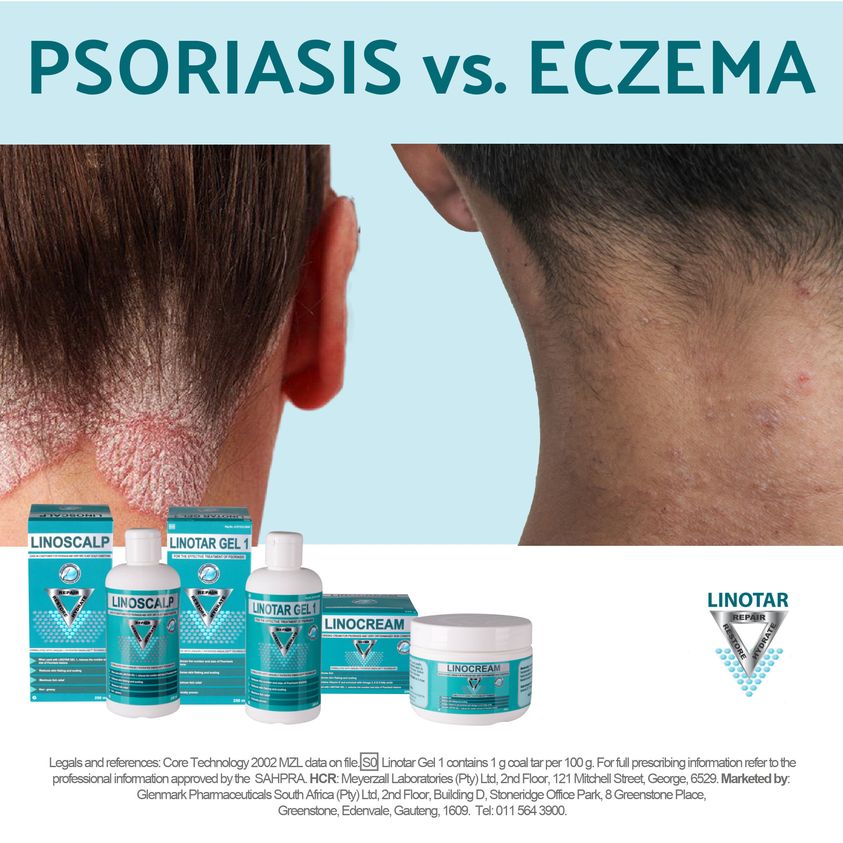
What is Eczema?
What is Eczema? What causes Eczema?
Eczema is also known as atopic dermatitis, or atopic eczema (the most common form of eczema). Atopic eczema mainly affects children, but it can continue into adulthood or start later in life. The word eczema comes from the Greek word ekzein meaning “to boil out”; the Greek word ek means “out”, while the Greek word zema means boiling.
Eczema is a chronic skin condition in which the skin becomes itchy, reddened, cracked and dry. Approximately 30% of all skin-related GP visits in Western Europe result in a diagnosis of atopic eczema. It affects both males and females equally, as well as people from different ethnic backgrounds. Most GPs (general practitioners, primary care physicians) in Western Europe, North America and Australia say the number of people diagnosed each year with eczema is has been rising in recent years.
Atopy is the hereditary predisposition toward developing some hypersensitivity reactions, such as hay fever, asthma, chronic urticaria, and some types of eczema. Atopic eczema, therefore, means a form of eczema characterized by atopy – in other words, inherited eczema.
Approximately 80% of atopic eczema cases start before the age of 5, and a sizeable number develops it during their first year of life.
What are the symptoms of eczema?
As atopic eczema is a chronic disease symptoms are generally present all the time. A chronic disease is a long-term one; one that persists for a long time. However, during a flare-up symptoms will worsen and the patient will probably require more intense treatment.
Below are some common symptoms of atopic eczema (without flare-up):
– The skin may be broken in places.
– Some areas of the skin are cracked.
– The skin usually feels dry.
– Many areas of skin are itchy, and sometimes raw if scratched a lot.
– Itching usually worse at night.
– Scratching may also result in areas of thickened skin.
– Some areas of skin become red and inflamed.
– Some inflamed areas develop blisters and weep (ooze liquid).
– The skin has red to brownish-gray colored patches.
– Areas of skin may have small, raised bumps.
Although the patches may occur in any part of the body’s skin, they tend to appear on the hands, feet, arms, behind the knees, ankles, wrists, face, neck, and upper chest. Some patients have symptoms around the eyes, including the eyelids. Scratching around the eyes may eventually lead to noticeable loss of eyebrow and eyelash hairs. Babies tend to show symptoms on the face.
When there is a flare-up the previous symptoms still exist, plus some of the ones below:
The skin will be much more itchy.
Itchiness and scratching will make the skin redder, raw and very sensitive.
Many of the affected areas will feel hot.
The skin will be much more scaly and drier.
The raised bumps will be more pronounced and may leak fluid.
Blisters will appear.
The affected areas may be infected with bacteria.
Flare ups can last from a day or two to several weeks.
Patients with mild atopic eczema will generally have only small areas of dry skin which may itch sometimes. When symptoms are severe large areas of skin become very dry and the itching is constant. Many areas will ooze fluid.
A vicious circle can set in. It starts with unpleasant itching, then scratching which makes the itching worse, which makes the patient scratch more – eventually the skin can bleed. Children who get into this cycle can suffer serious sleep disruption and may find concentrating at school extremely challenging.
The following may worsen the symptoms of atopic eczema:
– Prolonged hot showers or baths.
– Allowing the skin to stay dry.
– Mental stress.
– Sweating.
– Rapid temperature changes.
– Dry air.
– Certain fabrics for clothing, such as wool.
– Cigarette smoke.
– Dust.
– Sand.
– Some soaps, solvents, or detergents
A Swedish study found that linalool, the most common fragrance ingredient used in shampoos, conditioners and soap is a powerful allergen for a significant number of people.
What are the causes of atopic eczema?
Experts say that people with eczema are born with it – it is a genetically inherited condition. It can be worsened with exposure to external or environmental factors such as pollen or pet fur, and internal factors such as hormone levels and stress.
In 2006, scientists from the University of Dundee, with collaborators in Dublin, Glasgow, Seattle and Copenhagen, discovered the gene that causes dry, scaly skin and predisposes individuals to eczema.
In 2009 a study carried out by scientists at the University of Edinburgh concluded that the defects in a particular gene known as the filaggrin gene are linked to a considerably amplified risk of developing allergic disorders such as eczema, rhinitis, and asthma.
The oily (lipid) barrier of skin is usually reduced in people with atopic eczema, compared to other people. The lipid barrier helps prevent water loss. If your barrier is reduced you will lose water faster and your skin will be drier. Several studies have been confirming this, including this one.
The immune system cells of people with atopic eczema release chemicals under the skin’s surface which may cause inflammation. Experts are not 100% sure why this happens. They just know that it is an immune system overreaction.
Even though scientists are fairly sure genetics are the primary cause, they do not yet know what the exact genetic cause is. The above-mentioned studies are giving us a better idea – but a great deal of further research is needed. 60% of children with atopic eczema have one parent with the same condition. Studies have shown that children run an 80% risk of developing eczema if both their parents have the condition.
Eczema linked to gut bacteria in children – children who have eczema have a wider range of bacteria in their gut compared to kids without the condition, researchers from the University of Turku, Finland, reported in the journal BMC Microbiology. The scientists noticed that the bacteria in the gut of children with eczema were more like those found in adults than other kids.
Recent studies are starting to reveal a picture of early life lifestyle habits that may reduce the risk of developing eczema later on, either during early childhood or later on in life. An infant diet that includes fish before the age of 9 months curbs the risk of developing eczema, a Swedish study reported.
Environmental factors that make atopic eczema symptoms worse
Some scientists say that environmental factors are the ones causing the number of recent eczema cases in the developing world to rise. They argue that it is highly unlikely that genetic factors would change in such a short time.
Environmental factors are also known as allergens – they cause the body’s immune system to overreact; an allergic reaction.
The three most common allergens for atopic eczema are:
– House dust mites (bed bugs)
– Pollen
– Pet fur
Children who are exposed to cats soon after birth may have an increased risk of developing eczema, according to a study carried out by researchers at the University of Arizona in Tucson, USA.
These three allergens are also the main ones that trigger asthma and hay fever.
Hard water
Several scientists have suggested that hard water may be bad for people with eczema. Scientists from the University of Portsmouth, England, are carrying out a study to find out whether installing a water-softener in the home might improve the symptoms of children with eczema. Results of their study should appear around the end of 2009.
Foods that may make atopic eczema symptoms worse
These are foods that typically cause allergic reactions in people with sensitive immune systems. These include:
– Milk (cow’s)
– Eggs
– Nuts
– Soya
– Wheat
About 10% of children with atopic eczema are affected by food allergens. Foods rarely affect the symptoms of adults with eczema.
Hormones can worsen symptoms
A significant proportion of women with eczema report that their symptoms worsen during their menstrual cycle. 30% of women have flare ups during the days preceding their menstrual period. 50% of women with eczema say their symptoms got worse when they were pregnant. These are all periods when a woman’s hormone levels change.
Mental stress can make eczema symptoms worse
Doctors are not sure what exactly it is that causes a worsening of symptoms during mental stress. Atopic eczema patients commonly report that their symptoms are likely to get worse when they are mentally stressed. It is possible that a vicious cycle could develop – the symptoms of eczema stress the patient, the resulting stress exacerbates the symptoms, etc.
Winter is usually worse than summer
Most patient who do not live near the equator find that their symptoms are worse in the winter than the summer, even though pollen is an important trigger.
Diagnosis of eczema
No laboratory test or skin test currently exists which can diagnose atopic eczema.
A GP is able to diagnose atopic eczema after examining the patient and asking some questions about his/her symptoms and medical history – this will include questions about the presence of eczema in close family relative. The doctor will also ask about some other allergy-related conditions, such as asthma and hay fever.
A number of diagnostic criteria to confirm diagnosis
A doctor in the UK will assess the patient’s skin against a number of diagnostic criteria in order to confirm an eczema diagnosis. The criteria include:
A long period with itchy skin – the patient has had itchy skin for the last 12 months.
Plus at least three of the criteria below:
Itching and irritation – itchiness and irritation in skin creases, such as the front of elbows, behind the knees, front of ankles, around the neck, or around the eyes.
Asthma or hay fever – the patient either has asthma or hay fever or has had them in the past. If the child is under four, the doctor will ask whether a close relative (brother, sister, mother, father) has asthma or hay fever.
Dry skin – the patient’s skin has been dry for the last 12 months.
When it started – the condition started when the patient was two years old, or less. (If the patient is under four years of age this criterion is not used).
Joints – eczema is present either where skin covers the joints or the parts of the body that flex, such as wrists, knees, or elbows.
If the patient meets these criteria (the first, plus at least three of the others) the UK doctor will not usually have to carry out any further testing to confirm diagnosis.
Identifying trigger factors during diagnosis
The doctor will try to find out what triggers worsen the patient’s symptoms. He/she will ask the patient questions about lifestyle, soaps and detergents used, diet, home environment, pets, where exactly the house is, etc.
Some doctors will ask the patient to keep a diary – the patient will note down such data as eating habits, clothes worn, what time of day symptoms are better or worse and where the patient was during those times, etc. The aim here is to identify as many trigger factors as possible.
What is the treatment for atopic eczema?
There is currently no cure for atopic eczema – there is no treatment that gets rid of it for good, as might be the case with surgery to cure blindness caused by cataracts. However, there are a variety of treatments which focus on the symptoms, as well as strategies to avoid triggers, and may improve the patient’s quality of life considerably.
A significant proportion of children with atopic eczema will find that their symptoms will improve as they get older.
Self-care – What the patient can do
Avoid scratching
Itchiness is a common part of eczema, and scratching is a natural reaction to deal with itching. Unfortunately, scratching will invariably further aggravate the skin and make symptoms worse. Scratching also raises the risk of infection.
Getting an adult to control his/her scratching is hard enough – it is even harder for children. Children will often not be able to control the urge to scratch. It is important that nails are kept short and clean. Babies may benefit from anti-scratch mittens.
Avoid trigger factors
A good doctor will have established a list of factors that trigger eczema flares. The patient should try to avoid them as much as possible. Parents/guardians need to remind children of triggers and help them devise strategies to avoid them – younger children may need to be reminded frequently.
People with atopic eczema usually avoid clothes made of synthetic fibers and opt for natural materials, such as cotton.
We know that dust mites are likely triggers for many people. However, most studies have shown that trying to eradicate them from your home is very time consuming and does not seem to be very effective in reducing the frequency and severity of flare-ups. Several patients have written into Medical News Today saying that when they get up in the morning they pull their sheets right back and do not make their beds for several hours, allowing the bed to be ventilated – this has helped them (bear in mind this information is not a study, and must be taken as anecdotal).
Nutrition
It is important to check with your doctor before undergoing any large change in diet, especially if the patient is a child. Breastfeeding mothers whose babies have atopic eczema should check with their GP before embarking on any significant diet change. Milk, eggs, and nuts are common triggers. Researchers from King’s College London found no evidence that exclusive breastfeeding reduces the risk of a baby eventually developing eczema.
The German Institute for Quality and Efficiency in Health Care stresses that parents should be cautious about eliminating important foods like milk from their baby’s or child’s diet. In fact, their report says that avoiding foods may do more harm than good for children with atopic eczema, unless your child has a proven food allergy.
Regular fast-food consumption linked to eczema risk – children who consume fast foods at least three times a week are much more likely to have eczema as well as hay fever, researchers reported in the journal Thorax (January 2013 issue).
If you have identified the triggers you should avoid them. However, if a child’s trigger is milk he/she will need an alternative source of calcium. Always check with your doctor or a qualified nutritionist first before taking a major food source out of your or a child’s diet.
Complementary therapies
These are very popular among patients with atopic eczema. They include aromatherapy, massage, homeopathy, and some herbal remedies, to mention but a few. It is important to remember that although patients do report benefits, a lot of information one reads in books and on the internet is anecdotal. For therapy to be convincing, it should undergo proper clinical tests, usually carried out and compared to a placebo (dummy treatment). Before undergoing any complementary/alternative therapy, check it out carefully.
Researchers at Mount Sinai Hospital in New York reported that treatments consisting of Erka Shizheng Herbal Tea, a bath additive, creams and acupuncture, effectively treated patients with persistent atopic eczema. Their findings were presented at the 2009 Annual Meeting of the American Academy of Allergy, Asthma & Immunology.
Another study, carried out by Scientists at the Chinese University of Hong Kong, found that a traditional Chinese herbal concoction, consisting of Flos lonicerae (Japanese honeysuckle), Herba menthae (peppermint), Cortex moutan (root bark of peony tree), Atractylodes Rhizome (underground stem of the atractylodes herb) and Cortex phellodendri (Amur cork-tree bark) may help people with eczema and reduced their needs for medications.
Bleach baths
Researchers from the Northwestern University Feinberg School of Medicine reported that bleach baths offer an effective treatment for kids’ chronic eczema.
Emollients
An emollient is an agent that softens and smoothes the skin – it can be a cream, lotion or ointment. They keep the skin supple and moist. Emollients are an important part of atopic eczema treatment. The skin of people with eczema is usually dry; emollients help keep them moisturized, which helps prevent cracking and irritation.
Finding the right emollient may be a question of trial-and-error at first. The patient may have to try several different ones before hitting on a suitable one. Patients usually end up needing different types of emollients for different parts of their body.
Some emollients are specific for very dry skin, while others are aimed at less dry skin. Ointments are generally prescribed for drier skin, while creams and lotions are usually prescribed for other skin types.
It is not uncommon for patients to find that an emollient is not longer as effective as it used to be. Others may start experiencing skin irritation after long-term use. If either case happens to you or your child, you should see your GP.
Applying an emollient – apply smoothly to the skin, following the direction the hair grows. Do not rub it in as this may irritate the skin. Gently dry the skin after washing and apply the emollient as soon as the skin is dry. Emollients must not be shared.
Creams and lotions are generally used for red, inflamed areas.
Ointments are usually used for dry areas that are not inflamed.
Apply often – Frequency is the key for effective emollient use. Do not stop applying it when the skin seems to be clear. Frequent use on known affected areas will significantly reduce the number of flare-ups, as well as their severity. Patient’s whose skin is very dry should have repeat applications every two to three hours. During flare-ups frequency of use is paramount – this is when the skin needs the most moisture. Applications during a flare-up should be both frequent and generous.
If your child has atopic eczema it is important that you liaise with his/her school. In the UK it is common for a child to have emollient supplies at home and at school.
Emollient instead of soap – emollient treatments should be used in place of soap. Soap irritates the skin if you have atopic eczema. In many countries it is possible to purchase emollient bath and shower additives. This measure will make a significant difference in the patient’s frequency and severity of flare-ups.
Side effects of emollients – some patients may develop a rash with certain ingredients in a specific emollient. That is why people commonly have to try out different ones when they first start. Some emollients contain paraffin and can be a fire hazard – store them carefully and do not use them near a naked flame. Emollients may make the surface of the bath and the floor of the shower cubicle more slippery.
Topical corticosteroids
In medicine topical means “applied on to the skin”. Corticosteroids rapidly reduce inflammation. If the patient’s skin is very red and inflamed the doctor may prescribe a topical corticosteroid.
Many parents or adult patients react with alarm when the doctor utters any word with “steroid” in it. They imagine anabolic steroids that bodybuilders use. Corticosteroids are not anabolic steroids, and when used correctly, they are a safe and effective treatment for eczema.
Applying a corticosteroid – apply to the affected area sparingly. Follow the instructions on the leaflet carefully. You can also ask the doctor, and if you cannot remember, ask a qualified pharmacist.
Applying a corticosteroid during a flare-up – the corticosteroid should not be applied more than twice daily. Most patients will only require one application per day. After the flare-up has cleared up you should continue for another 48 hours.
If the patient is using corticosteroids on a long-term basis, he/she should check carefully with the doctor on how and when to apply it.
If you have tried corticosteroids and symptoms have not improved you should see your doctor.
Alitretinoin (Toctino)
Alitretinoin is used for patients with severe, chronic hand eczema who have not responded to other treatments. A specialist skin doctor (dermatologist) needs to supervise treatment with alitretinoin. Alitretinoin is a retinoid, a type of medication that helps lower levels of irritation and itchiness associated with eczema. Treatment usually consists of swallowing one tablet a day for 12 to 24 weeks.
Alitretinoin must NOT be taken by pregnant women or breastfeeding mothers. In most countries alitretinoin is not recommended for women of child-bearing age.
Side effects of alitretinoin include headaches, dry skin, flushed skin, joint pain, and muscle pain. The following extremely rare side-effects also exist: hair loss, blurred and distorted vision, and nose bleeds. Anybody who experiences blurred vision when taking this medication should contact the dermatologist immediately.
Antihistamines
This type of medication stops the effects of histamine, which our body releases when in contact with an allergen. If the effects of histamine can be stopped or reduced, symptoms of eczema, hay fever, and some other allergic conditions are often significantly reduced.
Sedating antihistamines can make some people feel drowsy and are generally prescribed for itchiness at night – their drowsiness side-effect will help some patients get a good night’s sleep. Sedating antihistamines are not usually prescribed for more than a couple of weeks at a time. They should be taken about one hour before going to bed. Sometimes drowsiness is still present the following day – it is important that the child’s school knows this. If the patient is an adult and feels drowsy the following morning he/she should not drive or operate heavy machinery.
Non-sedating antihistamines may be used on a long-term basis. They will help ease itching but will not make the patient feel drowsy.
Infection
If the eczema becomes infected the patient will probably need an antibiotic.
Oral antibiotic – An oral antibiotic will be prescribed if symptoms are very severe and infection has affected a large area. The most commonly prescribed antibiotic is flucloxacillin, which should be taken for seven days. If you or your child are allergic to penicillin a different antibiotic will be prescribed, perhaps erythromycin or clarithomycin.
Topical antibiotic – if symptoms are not so severe and the infection does not cover a large area the patient will most likely be prescribed a topical antibiotic – one that is applied directly onto the affected area. This will usually be an ointment or a cream.
The doctor may prescribe new supplies of topical medications in case your current ones have become infected.
Patients who have areas which are prone to recurrent infection may be prescribed a topical antiseptic, which is applied directly onto the targeted area of skin. Examples include chlorhexidine and triclosan.
Light Therapy (Phototherapy)
This involves the use of natural or artificial light. In its most simple form, all the patient has to do is expose himself/herself to controlled amounts of natural sunlight.
Other forms of phototherapy include using artificial ultraviolet A (UVA) or ultraviolet B (UVD) light, either on its own or in combination with drugs.
Light therapy is very effective. It is important that it is done with a qualified health care professional. Exposure to sunlight has many beneficial effects, but it does, however, also have risks if not controlled properly. Examples of risks include premature skin aging and a higher risk of developing skin cancer.
When to see a specialist
The GP may refer a patient to a specialist skin doctor (dermatologist) if:
– The patient has not responded to treatment.
– The GP is uncertain about what is causing the eczema.
– The patient insists the GP refers him/her or the child to a specialist.
– The GP thinks the patient would benefit from specialist treatment, such as ultraviolet light exposure, bandaging treatments (wet wraps), or calcineurin inhibitors.
Complications of atopic eczema
Infection
If the skin becomes dry and cracked there will be an opportunity for bacteria to penetrate. The likelihood of this happening is greater for people with eczema. Scratching the eczema increases the risk of infection further.
A bacterium called Staphylococcus aureus (S. aureus) commonly infects people with eczema. An infection with S. aureus will make the eczema much worse, causing increased redness, oozing of fluid and crusting of the skin, making it virtually impossible for the skin to heal naturally (without antibiotics).
Psychological effects
The mental stress of living with eczema can have a psychological impact on the sufferer, especially if it started very early in life. Children with atopic eczema are much more likely to have behavioral problems at school, compared to their peers who do not have it. Parents sometimes comment that their child with atopical eczema is much more clingy than their other children.
The stress can also come from other people. More than a quarter of patients with atopic eczema have been bullied or teased because of their skin condition, according to an international study.
Children with eczema frequently suffer from a lack of self-confidence. Family support and encouragement is a crucial factor in helping them overcome this. If your child’s self-confidence appears to be seriously undermined, talk to a health care professional, as well as the staff at his/her school.
Sleep problems
The majority of children with atopic eczema have sleep-related problems. Lack of sleep can have an impact on the patient’s physical and mental health.
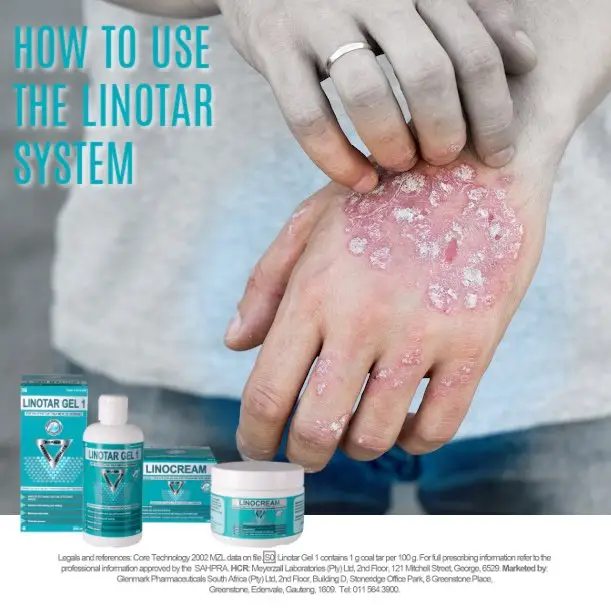
Brought to you by Linotar, in the interests of promoting an awareness about psoriasis and eczema. Linotar offers relief from the itch, burn and sting associated with psoriasis and eczema.
什么是湿疹?是什么原因导致湿疹?
湿疹也被称为异位性皮炎或异位性湿疹(湿疹的最常见的形式)。异位性湿疹,主要影响儿童,但它可以持续到成年或成年以后才发作。濕疹(eczema) 來自古希臘文ekzein, 意思是“沸騰而溢出”;希腊字EK意思是“出去”,而希腊字zema表示“沸騰”。
湿疹是一种慢性皮肤状况,会产生皮肤发痒、发红、破裂和干燥,在西欧大约30%的皮肤相关的医师门诊诊断出过敏性湿,湿疹对男性和女性的影响是同样的,对不同种族背景的影响也是一样,大多数在西欧、北美和澳大利亚的GPS(全科医生)指出;每年诊断患有湿疹的人数已经在最近几年有上升趋势。
遗传性过敏症是遗传性易患病的体质, 傾向发展某些過敏反應,如枯草熱、哮喘、慢性蕁麻疹,和某些类型的湿疹。异位性濕疹,因此,意味着濕疹的形式是以遗传性过敏为特征 , 换句话说就是,遗传的湿疹。
大约80%的过敏性湿疹在5岁之前就开始,相当数量的患者在一岁就形成了。
什么是湿疹的症状?
就如异位性湿疹是一种慢性疾病,它的症状通常一直存在,慢性疾病是一个长期性的; 持续很长一段时间。然而,急性发作期间症状会恶化,而且患者可能需要更强烈的治疗。
下面是过敏性湿疹的一些常见的症状(非急性):
皮肤有些地方会破皮。
皮肤有些地方会裂开。
皮肤通常会感觉干燥。
皮肤许多地方都发痒,如果搔抓太多有时皮肤会红肿。
发痒通常在夜间最严重。
抓挠也可能导致有些地方皮肤增厚。
有些地方变得发红和发炎。
有些发炎地方会有水泡和流脓(软泥液体)。
皮肤会有红至棕灰色的斑点。
皮肤有些地方可能有小的、凸起的肿块。
虽然斑块可能发生在身体皮肤的任何部位,他们往往出现在手、脚、胳膊、膝盖、脚踝、手腕、面部、颈部和上胸部,有些患者的症状会发生在眼睛周围,包括眼睑,眼睛周围的抓伤可能最终会导致眉毛和睫毛明显的减少,婴儿的症状往往显示在面部。
当急性发作,之前的症状仍然存在,还会加上一些下面罗列的症状:
皮肤会更痒。
瘙痒和搔抓会使皮肤更红,刺痛和非常敏感。
许多受感染的地方会觉得热。
皮肤会有更多鳞屑和更干燥。
凸起的肿块会更加明显,可能会漏出液体。
水泡会出现。
受感染的地方可能会被细菌感染。
急性发作可以维持一天或两天,到几个星期之久。
轻度过敏性湿疹患者,一般只有小面积的皮肤干燥,有时候会发痒。当症状严重变成大面积时, 皮肤会变得非常干燥,发痒会一持续,很多地方可能会渗出液体。
恶性循环会发生,从不愉快的瘙痒开始,搔抓会使发痒变得更糟糕,这让病人抓的更厉害 ,最终会使皮肤流血。小孩子进入这个循环,睡眠会受到严重干扰,也可能发现在学校,集中精神学习是很困难的。
下列情况可能使过敏性湿疹的症状恶化:
长时间热水淋浴或浴缸泡澡。
任由肌肤一直干燥。
精神压力。
出汗。
快速温度变化。
干燥的空气。
服装某些织物,如羊毛。
香烟烟雾。
灰尘。
沙子。
某些香皂,溶剂或清洁剂。
瑞典的一项研究发现,芳樟醇,是在洗发水、护发素和香皂中,最常用的香水成分,对相当多数的人而言,是一个功能强大的过敏原。
造成过敏性湿疹的原因是什么?
专家说,人类的湿疹是天生的 – 这是一种基因遗传条件。它可以被恶化,因为暴露于外部或环境因素;如花粉或宠物皮毛,和内部因素;例如荷尔蒙分泌和压力。
2006年,邓迪大学的科学家,在都柏林,格拉斯哥,西雅图和哥本哈根,发现导致干燥,鳞屑皮肤和个人易患湿疹的基因。
在2009年科学家在爱丁堡大学的研究得出结论,被称为聚角蛋白微丝基因的特定基因缺陷,是与相当地增大发生过敏失调的风险有关,如湿疹,鼻炎和哮喘。
在湿疹患者身的皮肤油性(脂质)屏障,和其他人相比,通常是减少的。脂质屏障有助于防止水分流失,如果你的屏障减少,你水分流失会更快,你的皮肤会干燥,许多研究已经证实这一点,包括这个研究。
异位性湿疹患者的免疫系统细胞,在皮肤表面下释放化学物质可能引起发炎,专家们不是100%肯定,为什么出现这种情况,他们只知道,这是一种免疫系统的过度反应。
尽管科学家们相当肯定遗传是主要的原因,他们还不知道确切的遗传原因是什么,上述研究是给我们一个更好的想法 – 但大量的进一步研究是必要的。60%的儿童的过敏性湿疹和父母其中一位的情况会相同,研究显示,如果父母双方都有这情况, 儿童就有80%的风险会得到湿疹。
芬兰图尔库大学研究人员在BMC微生物学杂志上发表,湿疹与儿童肠道细菌有关, 和没有湿疹的孩子相比,有湿疹的孩子肠道里有更多细菌,。科学家们发现,在湿疹儿童肠道的这种细菌,更容易在成人体内找到,比在其他孩子体内更容易找到。
最近的研究已经开始揭露,早期的生活习惯,可能降低以后发生湿疹的风险,无论是在儿童早期或以后的生活。一份瑞典的研究报告指出,婴儿饮食,包括9个月之前吃鱼,会抑制湿疹发作的风险。
环境因素导致异位性湿疹症状更严重
有一些科学家说:环境因素是造成近期在开发中国家许多湿疹案例增加原因,他们争论;基因因素不可能在如此短的时间就改变。
环境因素也被称为过敏原 – 它们会导致人体的免疫系统反应过度; 过敏反应。
三种过敏性湿疹最常见的过敏原:
屋尘螨(臭虫)
花粉
宠物皮毛
刚出生的婴儿暴露于猫当中,可能增加发生湿疹的风险,根据美国亚利桑那大学.图森市研究人员进行的研究,。
这三个过敏原也是主要的诱发哮喘和花粉症。
硬水
多位科学家认为硬水可能对患有湿疹的人是不好的,来自英国朴次茅斯大学的科学家,正在开展研究,以找出是否在家里安装软水机可以改善儿童患有湿疹的症状。他们的研究结果应该会在2009年年底提出。
食物,可能使过敏性湿疹症状变严重
这些食品通常会引起过敏反应,在有敏感的免疫系统的人身上。这些包括:
奶(牛的)
鸡蛋
坚果
黄豆
小麦
大约有10%的过敏性湿疹儿童是受到食物过敏原感染,食物很少影响成人湿疹的症状。
荷尔蒙可能加重症状
很大比例患有湿疹女性显示,他们在月经周期时症状恶化,30%的女性都在其月经期前几天爆发湿疹。50%有湿疹的女性,说在怀孕期间,她们的症状变得更糟。这些都是在当一个女人的荷尔蒙分泌发生变化的周期。
精神紧张可使湿疹症状加重
医生们不知道究竟是什么原因,导致精神紧张的时候湿疹症状会恶化,过敏性湿疹患者通常说,他们的症状在精神压力大时可能会恶化。这样的恶性循环是可能产生 – 湿疹带给患者压力,结果压力加剧了症状。
冬季通常比夏季更严重
大多数不生活在赤道附近的患者发现,自己的症状在冬天比夏天更糟糕,虽然花粉是一个重要的触发原因。
湿疹的诊断
现存的实验室试验或皮肤试验,没有可以诊断过敏性湿疹。
全科医生有能力诊断异位性湿疹,是透过检查和询问病患,他/她的症状和病史的一些问题, 包括家族亲戚有无湿疹。 医生还会问一些其他过敏相关的情况,例如哮喘和花粉热。
透过一些诊断标准,以确认诊断。
英国医生会將患者的皮肤对照一些诊断标准进行评估,以确认湿疹的诊断。该标准包括有:
长时间皮肤发痒 – 在过去12个月期间,患者有皮肤发痒情况。
加的至少下列的三个的标准:
发痒和刺激 – 瘙痒和红肿的皮肤皱褶,如肘部的前面、膝盖后方、脚踝的前面、脖子周围或眼睛周围。
哮喘或花粉症 -患者不是现在有哮喘或花粉症,就是以前得过。如果是四岁以下的小孩子,医生会问近亲(兄弟,姐妹,母亲,父亲)是否有哮喘或花粉症。
干性皮肤 – 过去12个月期间,患者的皮肤是干燥的。
什么时候开始有湿疹 – 患者在两岁或以下开始有湿疹。 (如果患者4岁年龄以下,就不适用这个标准)。
关节 – 湿疹不是出现在皮肤覆盖的关节,就是身体会弯曲的部位,如手腕、膝盖或肘部。
如果患者符合这些条件(第一项,加上至少其他三个标准)英国医生通常不会再进一步测试,就可以确认诊断。
诊断过程中识别触发因素
医生会尝试找出是什么触发因素让患者的症状恶化。他/她会询问患者的生活方式,使用什么肥皂和清洁剂、饮食、家居环境、宠物和房子确实的地点等问题。
有些医生会要求病人写日记 – 患者会记下饮食的数据、穿什么衣服、什么时候症状是好或是坏、发生这些症状的时候患者是在那里,目标是尽可能找出最多的触发因素。
用什么来治疗过敏性湿疹?
目前还没有过敏性湿疹治愈的药 – 没有任何的治疗是可以永远摆脱湿疹,就像手术治疗白内障引起的失明。但是,有多种针对症状的治疗方法,如同用策略避免触发湿疹一样,而且可以相当地改善患者的生活质量。
很大部分有过敏性湿疹的小孩会发现,他们的症状会因为随着他们长大而会有改善。
自我保健 – 病人可以做什么
避免搔抓
瘙痒是湿疹常见的症状,对付瘙痒,搔抓是一种自然的反应。不幸的是,搔抓会不约而同地进一步加害皮肤,使症状加重,抓痕也会引起感染的风险。
让一个成年人控制他/她的搔抓已经是很困难了 – 对小孩子更难。孩子们会常常无法控制冲动的搔抓,重要的是要保持剪短指甲和清洁, 戴抗划伤手套对婴儿可能会有助益。
避免触发湿疹因素
一位好的医生会建立一份触发湿疹因素的清单,患者应尽量避免接触,家长/监护人需要提醒孩子触发湿疹的因素是什么,帮助他们制定策略来避免 – 年幼的孩子可能需要经常提醒。
有过敏性湿疹的人通常要避免合成纤维制成的衣服,选择天然材料,例如棉质。
我们都知道,尘螨是很多人容易触发湿疹的因素。然而,大多数研究显示,你试图从你家消灭它们是非常耗费时间的, 也似乎并没有非常有效地减少湿疹发作频率和程度。好几位病人都写信给今日医学新闻说:当他们早上起床,他们会拉好他们的床单,而且几个小时内不整理他们的床,使床通风 – 这有助于他们(请记住此信息不是一个研究,而且必须被视为轶事)。
营养
进行任何重大的饮食改变,咨询您的医生是很重要的,尤其是如果患者是儿童。哺乳中母亲的婴儿有过敏性湿疹,在进行任何重大的饮食改变前,请咨询您的医生。牛奶,鸡蛋和坚果是常见的触发因素。来自伦敦国王学院的研究人员发现,没有证据显示哺喂母乳会降低婴儿最终发生湿疹的风险。
德国质量和效率卫生保健机构强调,家长应谨对待有关删除他们的婴儿或儿童的饮食上重要的食物,如牛奶。 事实上,他们的报告中说明,对有过敏性湿疹的儿童,避免吃那些食物可能是弊大于利,除非你的孩子已经被证明有食物过敏。
定期速食消费与湿疹风险的关联; 研究人员发表在Thorax杂志(2013年1月号), 一个星期购买速食至少三次的孩子,更容易有湿疹和花粉症,。
如果你已经确定什么是触发因素,你应该避免它。然而,如果一个孩子的触发因素是牛奶,他/她将需要补钙的替代来源,在拿掉你的或是你小孩的主要食物来源之前,咨询你的医生或合格的营养师,
辅助疗法
有一些治疗方法在过敏性湿疹患者中很受欢迎, 包括芳香疗法、按摩、顺势疗法,以及一些草药,仅举几例。重要的是要记住,虽然说对患者有好处,书上和网路上大量的信息是轶事。治疗要有说服力,应进行适当的临床试验,通常进行和比较一种试验药物用的无效对照剂 (虚拟治疗),在接受任何补充/替代治疗之前,都需要仔细检查。
在纽约西奈山医院的研究人员提出, 治疗包括用Erka Shizheng凉茶,洗澡添加剂,面霜和针灸,有效治疗了持续过敏性湿疹的患者。他们的研究结果发表在2009年美国学院的过敏哮喘和免疫学的大会上。
另一项研究是由在香港中文大学的科学家开展,发现中国传统的中药调和物,包含金银花(日本金银花),薄荷(薄荷),牡丹皮(牡丹树的根皮),苍术属(地下茎的草本植物白术)和黄柏(黑龙江软木树皮)可能会帮助改善人们的湿疹和减少他们对药物的需求。
漂白浴
西北大学医学院的研究人员报告提出, 漂白浴提供患有慢性湿疹的儿童一种有效的治疗。
润肤剂
润肤剂是软化和平滑皮肤的药剂 – 它可以是乳膏剂、乳液或软膏。它们是用来保持肌肤水嫩滋润,润肤剂是过敏性湿疹治疗的重要部分。患有湿疹的皮肤一般是干燥的,润肤剂有助于保持皮肤的滋润,这有助于防止皮肤开裂和刺激。
找到合适的润肤剂起初可能要不断尝试,病人在找到适合的润肤剂之前,必须要尝试几种不同的润肤剂。一般患者通常最后是针对自己身体的不同部位,需要不同类型的润肤剂。